
Prior authorization is already a fight. Federal AI governance just made the rules more complicated.
What Federal AI Policy Means for Community Oncology Practices Right Now
Prior authorization is already a fight. Federal AI governance just made the rules more complicated.
Community oncology practices are increasingly expected to respond to AI-assisted utilization management systems without equivalent visibility, staffing, or technical leverage. Payers are automating denial logic and independent clinics are absorbing the downstream labor burden. That asymmetry is what makes the current governance moment consequential, not the technology itself.
The problem is not that AI is coming. The problem is that payers are deploying it first. Community practices are absorbing opaque, AI-driven denial behavior without equivalent tools to identify it, challenge it, or document it. That structural imbalance is the real governance issue, and federal policy has not yet resolved it.
In January 2025, Executive Order 14179 directed federal agencies to cut regulatory friction on AI development and prioritize American competitiveness in the field. At first that sounds like less oversight. In practice, however, it means AI deployment in healthcare will accelerate while formal regulatory guardrails lag. The burden of defining what “responsible AI” looks like in prior authorization will fall increasingly on payers, vendors, and the contracts your practice signs.
That is a meaningful shift in risk.
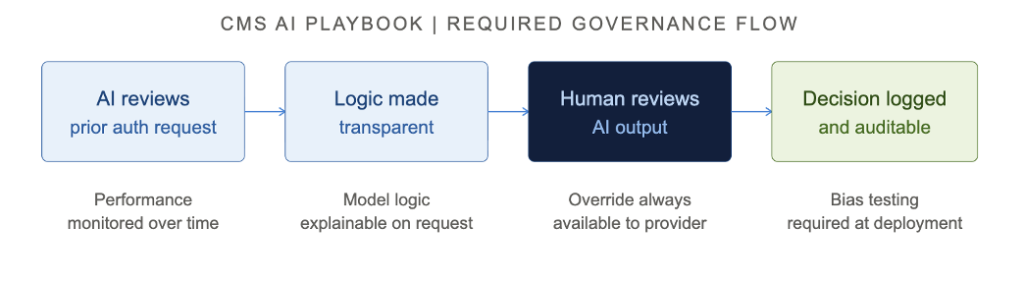
CMS released Version 4 of its AI Playbook in 2025, laying out the agency’s internal principles for AI governance. AI tools affecting coverage decisions must be transparent in their logic, monitored for performance over time, and designed with human oversight at critical decision points. The playbook also establishes a graduated risk evaluation model, where high-stakes AI tools face stricter scrutiny before deployment.
For community oncology practices, this matters in two ways. First, it signals that any AI tool a payer deploys in the prior authorization process should meet these standards. Second, it gives your practice a framework to evaluate the vendors you work with. If a vendor cannot explain how their model makes decisions or demonstrate ongoing performance monitoring, that is a red flag.
Auditability and explainability are not abstract standards. For a community oncology practice, they are practical requirements. When a payer’s AI system denies a chemotherapy authorization, your team needs to know specifically: what rule triggered the denial, what policy version was applied, whether that payer logic changed recently, and whether the denial was algorithmically generated or flagged for human review. Those are not unreasonable questions. They are the minimum information required to mount a competent appeal. Traceable decision pathways, documentation retention, versioned policy logic, and appeal traceability belong in every vendor and payer agreement your practice signs. When an AI-generated denial delays medically necessary oncology treatment, accountability for that outcome is not optional. It instead belongs in the contract. Practices that cannot get that information from their vendors or from payers are operating blind, and that exposes them on both the revenue and the compliance side.
The Community Oncology Alliance filed formal comments urging CMS and HHS to develop governance standards that protect independent practices from unchecked payer-deployed AI. Their position is direct: AI used in prior authorization must be clinically validated, transparent in its logic, and subject to provider override. Payers cannot deploy a black-box algorithm that denies complex oncology authorizations and hide behind automation.
COA has also raised a concern that does not get enough attention. Small and independent practices risk falling behind not because they refuse AI, but because they lack the infrastructure and bandwidth to deploy it. Large health systems will absorb these tools quickly while community clinics face AI-driven payer decisions without AI-assisted responses. That gap in capability becomes a gap in revenue, and a change in how these clinics can operate. Consider what that looks like in practice: a community oncology clinic submits a prior authorization for a mutation-targeted therapy, the payer’s automated system flags it for missing biomarker documentation, the denial arrives with no explanation of which specific result was required or which policy version triggered the flag, and the staff member responsible for the appeal has no way to determine whether the criteria changed since the last submission. That is not a technology failure. That is an accountability failure, and it is happening now.
As formal AI regulation lags deployment, the contract is where governance actually happens. For community oncology practices, that means vendor and payer agreements need to address four things explicitly.
Data ownership: who owns the derived workflow intelligence your practice generates, and can a vendor retrain its models on your patient interaction data?
Liability allocation: when an AI-generated denial delays a medically necessary treatment, where does operational responsibility begin and where does vendor accountability end?
Model drift monitoring: in oncology, payer criteria, NCCN alignment, biomarker requirements, and treatment pathways change continuously. A static AI model that is not actively recalibrated against those changes becomes unreliable without anyone flagging it.
And human override authority: any AI tool operating in prior authorization must support physician review, escalation rights, and peer-to-peer workflows. Override is not an edge case. It is a clinical requirement.
These are no longer edge-case procurement questions. They are the standard of care for evaluating any AI vendor that touches authorization workflows in oncology.
A 2025 policy brief published in NPJ Digital Medicine made the case that Medicaid’s prior authorization processes are delaying treatment for the patients who need it most. For oncology practices with a significant Medicaid census, that is not a policy abstraction. Authorization delays for chemotherapy regimens, infusion therapies, and supportive care drugs are days lost between diagnosis and first infusion, staff hours spent on manual documentation instead of patient care, and denial rates that do not reflect clinical need.
For community oncology practices, the immediate issue is not theoretical AI modernization at CMS. It is whether payer-side automation increases treatment delays and staffing burden faster than practices can adapt.
AI in prior authorization is moving faster than governance can keep up. Payers will deploy it. The practices that are protected are the ones that understand the rules, have vendor partners who meet them, and have automation in place to respond to AI-driven decisions at the same speed they arrive.
Three things to act on now. Review every vendor contract that touches prior authorization for transparency, override provisions, and the data governance terms discussed above. Ensure your RCM team understands the CMS AI Playbook benchmarks as a baseline for evaluating payer behavior. And document your authorization workflows thoroughly, because audit defensibility will matter more, not less, as AI becomes embedded in the denial process.
The practices that treat this as a policy update to file away will feel the consequences in their A/R days. The ones that treat it as an operational, governance, and contract management issue will be better positioned to protect revenue and keep patients on schedule.
Community Oncology Alliance. (n.d.). COA comments on accelerating the adoption and use of artificial intelligence as part of clinical care. https://mycoa.communityoncology.org/publications/comment-letters/coa-comments-on-accelerating-the-adoption-and-use-of-artificial-intelligence-as-part-of-clinical-care-rfi
Centers for Medicare & Medicaid Services. (2025). CMS AI playbook (Version 4). U.S. Department of Health and Human Services. https://ai.cms.gov/CMS-AI-Playbook.pdf
National Artificial Intelligence Initiative Act of 2020, Pub. L. No. 116-283, 134 Stat. 3388 (2021). https://www.congress.gov/116/crpt/hrpt617/CRPT-116hrpt617.pdf#page=1210
Executive Order No. 14179, 90 Fed. Reg. 8741 (January 23, 2025). Removing barriers to American leadership in artificial intelligence. https://www.whitehouse.gov/presidential-actions/2025/01/removing-barriers-to-american-leadership-in-artificial-intelligence/
Favini, N., Bhatt, J., & Navathe, A. S. (2025). AI-first Medicaid: How CMS can build a smarter safety net with precision benefits. NPJ Digital Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC12663265/
Author(s):
Joshua Upshaw, PhD
Co-Founder, CEO, Principal Investigator | Hidalga Technologies, Inc.
Elizabeth Grace Schmidt, MCS
Software Engineer, Medical Coder, Marketing and Analytics Manager, Hidalga Technologies, Inc.
Reviewed with input from:
Jeff Hunnicutt, CEO, Highlands Oncology
This article is published by Hidalga Technologies, Inc., an Arkansas based healthcare science and technology company building intelligent, clinically aligned workflow optimization systems for specialty medical practices.
© 2026 Hidalga Technologies, Inc. All rights reserved.
Reproduction or redistribution of this content without written permission is prohibited. For reprint or citation inquiries, contact@hidalgatech.com.